- Case Scenario Single White Female A 55 Year Old White Female Not Married Presented To The Emergency Department With A 1 (65.15 KiB) Viewed 48 times
- Case Scenario Single White Female A 55 Year Old White Female Not Married Presented To The Emergency Department With A 2 (35.73 KiB) Viewed 48 times
- Case Scenario Single White Female A 55 Year Old White Female Not Married Presented To The Emergency Department With A 3 (36.49 KiB) Viewed 48 times
CASE SCENARIO: Single White Female A 55-year-old white female, not married, presented to the emergency department with acute onset shortness of breath. Symptoms began approximately 2 days before and had progressively worsened with no associated, aggravating, or relieving factors noted. She had similar symptoms approximately 1 year ago with an acute, chronic obstructive pulmonary disease (COPD) exacerbation requiring hospitalization. She uses BPAP ventilatory support at night when sleeping and has requested to use this in the emergency department due to shortness of breath and wanting to sleep CODE She denies fever, chills, cough, wheezing, sputum production, chest pain, palpitations, pressure. abdominal pain, abdominal distension, nausea, vomiting, and diarrhea. She reports difficulty breathing at rest, forgetfulness, mild fatigue, feeling chiled, requiring blankets, increased urinary frequency, incontinence, and swelling in her bilateral lower extremities that are new-onset and worsening Subsequently, she has not ambulated from bed for several days except to use the restroom due to feeling weak, fatigued, and short of breath There are no known il contacts at home. Her family history includes significant heart disease and prostate malignancy in her father. Social history is positive for smoking tobacco use at 30 pack years She quit smoking 2 years ago due to increasing shortness of breath. She denies all alcohol and illegal drug use. There are no known foods, drugs, or environmental allergies Past medical history is significant for coronary artery disease, myocardial infarction COPD. hypertension, hyperlipidemia, hypothyroidism, diabetes mellitus. peripheral vascular disease. tobacco usage, and obesity. Past surgical history is significant for an appendectomy. cardiac catheterization with stent placement, hysterectomy, and nephrectomy Her current medications include fluticasone-vilanterol 100-25 meg inhaled daily, hydralazine 50 mg by mouth, 3 times per day, hydrochlorothiazide 25 mg by mouth daily, albuterol-ipratropium Inhaled every 4 hours PRN, levothyroxine 175 mog by mouth daily, metformin 500 mg by mouth twice per day, nebivolol 5 mg by mouth daily, aspirin 81 mg by mouth daily. Vitamin D3 1000 units by mouth daily, clopidogrel 75 mg by mouth daily, isosorbide mononitrate 60 mg by mouth daily, and rosuvastatin 40 mg by mouth daily Physical Exam Initial physical exam reveals temperature 97.3F, heart rate 74tom, respiratory rate 24cpm BP 104/54mmHg, BMI 40.2 and O, saturation 90% on room air. Appearance: Extremely obese, acutelyih-appearing female Well-developed and well-nourished with BiPAP in place. Lying on a hospital stretcher under 3 blankets. HEENT: • Hond: Normocephalic and atraumatic • Mouth: Moist mucous membranes • Macroglossia • Eyes Conjunctiva and EOM are normal. Pupils are equat, round, and reactive to light. No scleral icterus. Bilateral periorbital edema present. • Neck Neck supple. No JVD present. No masses or surgical scarring • Throat: Patent and most Cardiovascular: Normal rate, regular rhythm, and normal heart sound with no murmur. 2 pitting edema bilateral lower extremities and strong pulses in all four extremities. Pulmonary Chest: No respiratory status distress at this time, tachypnea present. (*) wheezing noted, bilateral rhonchi decreased air movement bilaterally. Patient barely able to finish a full sentence due to shortness of breath Abdominal: Son. Obese Bowel sounds are normal. No distension and no tenderness Skin Skin is very dry Neurologic: Alert, awake, able to protect her airway. Moving all extremities. No sensation losses
11:12 a 2 File Details NCMB418 RLE - BSN 4-Y1-RR 1 Installation to elucidate the source of Gyan was performed and included the an infectious of our was present CMP to Tectrolyte and review function and arterial blood gas to determine the POR for hypoca and any morale derangement, creatinine kinase and troponin to evaluate the presence of myocardial actor Habdomy brain ratture per ECG. and chest x cay Coming a wire and fuerzas endemic in the community and assay was obtained Laboratory and Diagnostics Her Chowed largely remarkable and non-contributory to establisha diagoa Chowd creatinine sevation store in from 10 to 151. Indicating posible acute EGFR 28 consistent with chronic mal das Cicin was eated 102 How when comeded for abumin is corrected to 0.8 mil Midratante presentine hosph. AST. ALT mement which could be due to the corn from our verload Intial arterial blood gas with H7491, PCO2 276. PO2 536. COS 20.6. and orygen saturation 90% on room indicating respiratory with hypocres Creatinine kinase was elevated wong with a varied broonines. In the setting of her known chronic ronalur and auto injury indicated by the storie van a trial thadors determined Infera And Negative ECG Normal rythmwth non peccst changes in interior do Decremet volgens IVR VL VF Chest X-ray Findingsbasilar airspaces that may represent alveolare Cardiolytted Prominent interstil markings noted Smak batera pleureusions Radiologist impression Radiographic changes of congestive tailure we boterapeutions greater on the le compond to nei Tasks 1 Develop a composed as a guide for the plan of care for the dent. You may use the concept map format shown below 2. Present the output during the synchronous SIGNANT DATA Previous Next D V Dashboard Calendar To Do Notifications Inbox
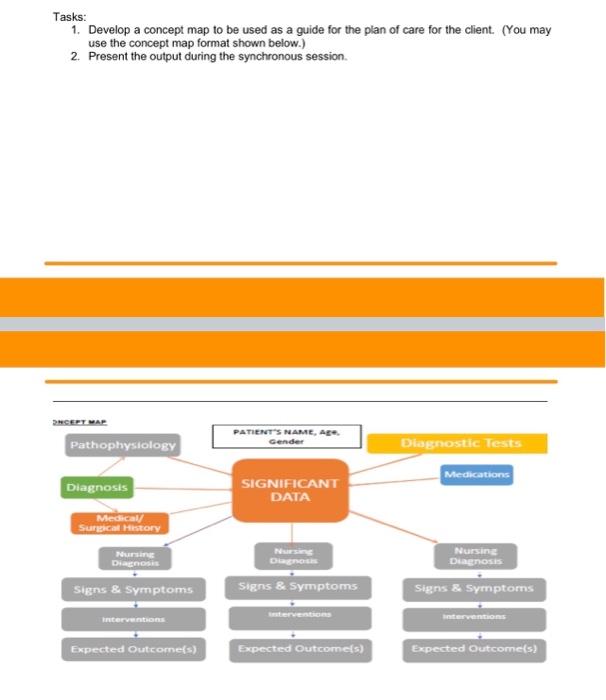
Tasks: 1. Develop a concept map to be used as a guide for the plan of care for the client. (You may use the concept map format shown below.) 2. Present the output during the synchronous session. PHCEPT WAP Pathophysiology PATIENT'S NAME, Age Gender Diagnostic Tests Medications Diagnosis SIGNIFICANT DATA Medical Surgical History Nursing Diagno NES D Nursing Diagnosis Signs & Symptoms Signs & Symptoms Signs & Symptoms ON interventions terventions eventos Expected Outcomes) Expected Outcomes) Expected Outcomes)